- News |
-
- Featured
-
Canada’s privacy commissioner launches investigation over the use..
As the years pass by, technology also widens, and more and more are being discovered. From simple gadgets..
- Business |
-
- Featured
-
Be an informer to I-T dept; earn up..
Sharing "specific information" with the income tax department about any benami..

- Tech & Industry |
-
- Featured
-
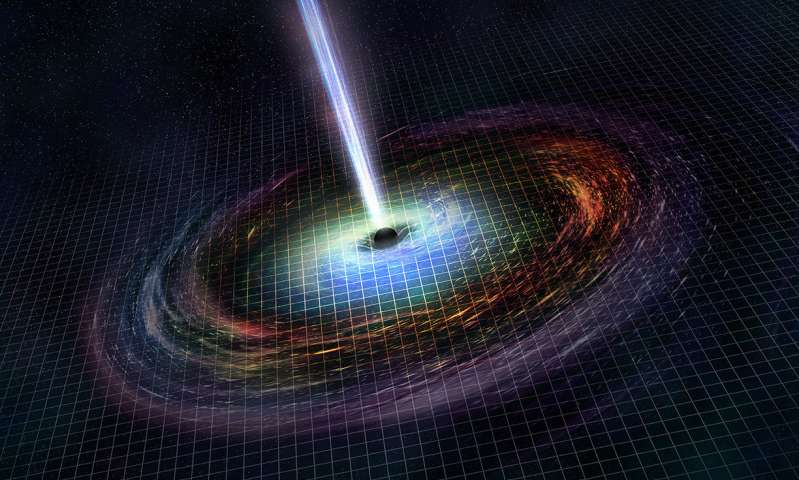
Gravitational wave event likely signaled birth of black..
The merger of two neutron stars that generated gravitational waves detected last year may have led to the birth..
- Entertainment |
-
- Topics
- Malayalam Film
- Media
- Music
- Youth
-
- Featured
-
Shawn Mendes Released Highly Anticipated Self-Titled Album Today
Los Angeles, CA : Multi-Platinum singer/songwriter Shawn Mendes released his highly anticipated self-titled third album today, via Island Records. Get..
-
- New Products |
-
- Topics
- General
-
- Featured
-
ZOTAC Introduces Its GeForce GTX 960 series graphics..
Dubai- ZOTAC International, a leading innovator and manufacturer of graphic cards and mini-

-
- Education |
-
- Topics
- Campus News
-
- Featured
-
ITM University, Gurgaon Student Palash Chhabra Represents Varsity..
New Delhi: Palash Chhabra, a student of ITM University,..

-
- Health |
-
- Topics
- Medical News
-
- Featured
-
Maharshi Shushruta, The Great Grandfather of Surgery!
by Ayurvedacharya Dr.Hitesh Jani Dr.Hitesh Jani
-
- Tourism |
-
- Topics
- Travel
- Food&Beverages
- Hospitality
-
- Featured
-
“Keraliya Ayurveda is Credible and Authentic”
Irina Gurjeva Irina Gurjeva is not just another vacationer in..

-
- Sports |
- Editor's column |
- Magazine |
Fibroids in Women
Published on April 5, 2013
Fibroids are solid balls of muscle that grow within the wall of the uterus or in its cavity, and they are extremely common. About 70 percent of women get them during their reproductive years, though only 25 percent experience symptoms like heavy menstrual periods. For this reason, most fibroids, also called leiomyomas, go undetected.
percent of women get them during their reproductive years, though only 25 percent experience symptoms like heavy menstrual periods. For this reason, most fibroids, also called leiomyomas, go undetected.
A single fibroid can be less than 1 inch in size or can grow to 8 inches or more. Fibroids usually pose little health risk, and most women have no problems with fertility. The growths usually shrink after menopause when there is little estrogen to fuel their growth. Hormone replacement therapy, however, can negate this effect and may not be advised for those experiencing symptomatic fibroids.
Often called “tumors,” fibroids are rarely cancerous. Symptoms may occur if the growths are in a certain location or reach a certain size. For example, those that grow in the cavity of the uterus usually cause bleeding between periods and often cause severe cramping. Those that grow partially within the wall and partially within the uterus can cause heavy periods, while those that grow completely within the wall may not cause any symptoms.
Diagnosis is usually made during a pelvic exam and can be confirmed through an ultrasound. Treatments vary depending on a woman’s age and her severity of symptoms. If a woman is near menopause, a “wait and see” approach might be all that’s needed. Certain medications may also be prescribed to help shrink the growths. Surgeries that remove just the fibroid or a hysterectomy to remove the uterus might be necessary for those plagued by heavy bleeding and painful cramping.
Need to Know Anatomy
The uterus is a hollow, 3.5 inch-long muscular organ that lies in a woman’s pelvic region and expands during pregnancy to accommodate the fetus. Shaped like an inverted pear, it lies between the bladder and the rectum and sits above the vagina. The lower narrow portion at the bottom is called the cervix, which protrudes into the vagina. The uterine tubes, or fallopian tubes, extend from either side of the uterus and serve as a pathway for eggs to travel from the ovary into the uterus.
Most fibroids grow within the wall of the uterus and are categorized into three groups depending on where they grow.
Submucosal fibroids grow just beneath the uterine lining and bulge into the cavity
Intramural fibroids grow inside the muscular wall of the uterus
Subserosal fibroids bulge toward the outside of the uterus
About 95 percent of the growths are found in the outer and middle layers of the uterus, while only 5 percent are in the inner submucosal tissue. Some fibroids grow on stalks and extend outward from the surface of the uterus or into the cavity.
Causes
Little is known about the cause of fibroids. A number of theories exist, but none provides a full explanation of what triggers them. Most likely, they result from a combination of factors, including genes and hormones.
Hormones: Strong evidence suggests that the female hormones estrogen and progesterone play a key role in promoting the growth of fibroids. In the presence of high levels of estrogen, fibroids can grow several inches in diameter. Fibroids also grow in the presence of progesterone and shrink with progesterone suppressors like the drug RU-486 (mifepristone). Other hormones such as growth hormone and prolactin are also thought to promote the growth of fibroids, though how much of a role they play remains uncertain.
Genes: While hormones fuel the growth of fibroids, genes may actually cause them to develop in the first place. Recent studies suggest that women with a family history of fibroids are twice as likely to develop the masses as those with no family history. Other research has found that it’s more likely that both identical twins with fibroids will need a hysterectomy than that both fraternal twins will. And recently, researchers at Brigham and Women’s Center for Uterine Fibroids have identified mutations in two genes, HMGI(C) and HMGI(Y), which appear to be important in the development of some fibroids.
Risk Factors
Fibroids are two to five times more prevalent in black women than in white women. Risk is also higher in women who are overweight and lower in those who smoke and those who have given birth. The relationship between fibroids and oral contraceptive use is complex. Oral contraceptives are thought to decrease the risk of developing fibroids, except in women who start using them before age 17. In general, there are no tried-and-true ways to prevent fibroids.
Fibroidlike Conditions
Certain uterine conditions can mimic the symptoms of fibroids. One such condition is adenomyosis, in which glandular tissue from the uterine lining migrates into its wall. About 20 percent of women are estimated to have this condition, and the vast majority of those have previously given birth. Although the exact cause is unknown, it seems to occur when the barrier between uterine layers breaks down.
About 60 percent of women with adenomyosis experience abnormal uterine bleeding, such as heavy periods or bleeding between periods, and 25 percent have severe pelvic pain with menstruation. There are no good diagnostic tests to detect the condition. Most of the time, adenomyosis is discovered during a hysterectomy to treat other conditions like fibroids. The only treatment is a surgical removal of the uterus since medications haven’t shown to be useful for controlling symptoms long term.
Endometrial polyps can also masquerade as fibroids. These are localized overgrowths of endometrial tissue that project into the uterus. They rarely occur in women under 20 and increase in prevalence with age until menopause when they usually resolve. About 10 to 24 percent of women undergoing hysterectomies have these polyps, which can cause heavy periods and bleeding between periods. Diagnosis can be made through an endometrial biopsy or dilation and curettage (D&C) procedure that dilates the cervix to obtain a sample of uterine lining. Ultrasound can also be useful in making a diagnosis. A newer technique called a hysteroscopy introduces a small tube with a camera attached through the vagina and into the uterus. The instrument can also obtain a biopsy sample. Treatment usually involves a D&C in which the polyps are removed by cutting away part of the uterine lining.



