- News |
-
- Featured
-
Canada’s privacy commissioner launches investigation over the use..
As the years pass by, technology also widens, and more and more are being discovered. From simple gadgets..
- Business |
-
- Featured
-
Be an informer to I-T dept; earn up..
Sharing "specific information" with the income tax department about any benami..

- Tech & Industry |
-
- Featured
-
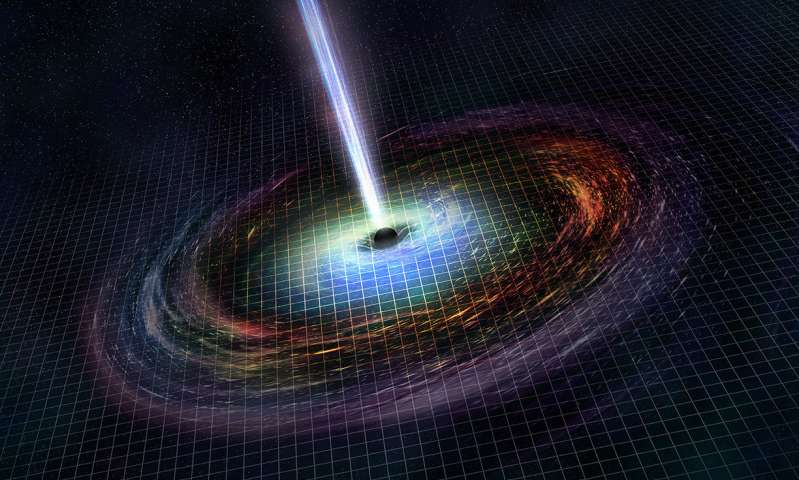
Gravitational wave event likely signaled birth of black..
The merger of two neutron stars that generated gravitational waves detected last year may have led to the birth..
- Entertainment |
-
- Topics
- Malayalam Film
- Media
- Music
- Youth
-
- Featured
-
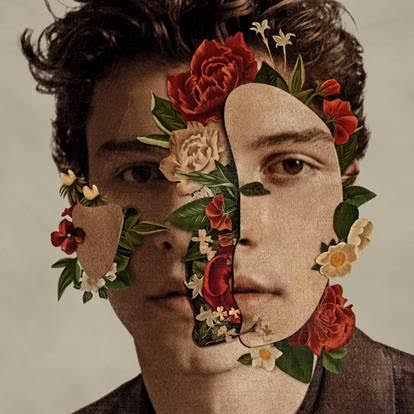
Shawn Mendes Released Highly Anticipated Self-Titled Album Today
Los Angeles, CA : Multi-Platinum singer/songwriter Shawn Mendes released his highly anticipated self-titled third album today, via Island Records. Get..
-
- New Products |
-
- Topics
- General
-
- Featured
-
ZOTAC Introduces Its GeForce GTX 960 series graphics..
Dubai- ZOTAC International, a leading innovator and manufacturer of graphic cards and mini-

-
- Education |
-
- Topics
- Campus News
-
- Featured
-
ITM University, Gurgaon Student Palash Chhabra Represents Varsity..
New Delhi: Palash Chhabra, a student of ITM University,..

-
- Health |
-
- Topics
- Medical News
-
- Featured
-
Maharshi Shushruta, The Great Grandfather of Surgery!
by Ayurvedacharya Dr.Hitesh Jani Dr.Hitesh Jani
-
- Tourism |
-
- Topics
- Travel
- Food&Beverages
- Hospitality
-
- Featured
-
“Keraliya Ayurveda is Credible and Authentic”
Irina Gurjeva Irina Gurjeva is not just another vacationer in..

-
- Sports |
- Editor's column |
- Magazine |
Bridging Hope: Addressing Birth Defects in India
Published on January 26, 2024

By Dr. C Priyamvada Reddy, Senior Consultant Obstetrician & Gynaecologist, Ankura Hospital
Birth defects, encompassing structural, functional, and metabolic abnormalities present from birth, have emerged as a significant cause of infant mortality in developing countries, including India. Despite substantial reductions in overall infant mortality, birth defects contribute significantly to this issue, with 70% being preventable through cost-effective community genetic services.
There are certain risk factors which are the root cause for birth defects. They are as follows: –
Advanced Maternal Age and Down Syndrome Incidence: The National Family Health Survey 3 (NFHS 3) notes that fertility rates among women aged 35-49 are around 53 live births per 1000 females. This is significant as advanced maternal age, constituting 17% of the female population, is associated with a higher incidence of Down syndrome. The estimated annual birth of Down syndrome babies in India is around 37,000, highlighting the need for targeted interventions for this demographic.
Antenatal Care Disparities: The NFHS 3 highlights a concerning lack of timely antenatal care, with 22.8% of pregnant females not receiving any care and 33% receiving care after 4 months. This delayed initiation of care leaves pregnancies vulnerable during the crucial period of organogenesis, contributing to preventable birth defects.
Maternal Lifestyle Factors: The prevalence of tobacco use (11%) and alcohol consumption (2.2%) among reproductive-age females is alarming. The association between maternal smoking and alcohol consumption during pregnancy and an increased risk of multiple birth defects underscores the need for targeted public health campaigns addressing these modifiable risk factors.
Consanguineous Marriages: Consanguinity rates ranging from 1% to 50% in different regions of India contribute to a higher risk of congenital malformations and genetic disorders. Prioritizing genetic counselling and carrier screening for couples in consanguineous marriages is essential.
Genetic Carrier Status: The carrier frequencies for genetic disorders like thalassemia and sickle cell anaemia are notably high among Indians. This emphasizes the need for a national program focusing on these conditions, incorporating carrier testing and prenatal diagnosis for at-risk couples.
Maternal Nutritional Deficiencies: NFHS 3 indicates that 51% of households use adequately iodized salt, while 55% of women are anaemic. Maternal deficiencies in iodine and folic acid are associated with birth defects. Thus, there is a crucial need for sustained efforts in promoting adequate nutrition and fortification programs.
Exposure to Teratogens: The exposure to teratogens, such as tobacco (11%) and alcohol (2.2%), during pregnancy is concerning. Efforts to raise awareness about the risks associated with these substances and implementing strict guidelines for their use during pregnancy are imperative.
Interventions:
Preconceptional Care: Preconception provides an opportune moment for implementing interventions focused on nutrition and other lifestyle factors. This ensures effective preparedness for pregnancy, promoting the health of both mothers and babies. Among adolescents, prevalent challenges include malnutrition and early pregnancy, especially in low- and middle-income countries (LMICs) where 99% of maternal and newborn deaths transpire. Unfortunately, these girls often receive minimal attention until their initial pregnancy, and subsequent interventions post-pregnancy are frequently insufficient to undo any adverse health impacts.
Preimplantation Genetic Testing (PGT) is a method employed in invitro fertilization (IVF) to identify genetic defects in embryos before pregnancy. Preimplantation Genetic Diagnosis (PGD) focuses on embryos when one or both parents have a known genetic abnormality. In contrast, Preimplantation Genetic Screening (PGS) examines embryos from presumed chromosomally normal parents for aneuploidy. PGT and PGS are the sole options available to reduce the risk of having a child with a genetic disease before implantation, offering an attractive alternative to dealing with the complexities of pregnancy termination following an unfavourable prenatal diagnosis.
Sometimes the couples ignore the tests prescribed to identify deformities in foetus, this removes any chance of timely intervention to correct birth defects. We at Ankura Hospital strongly recommend expecting parents to take the diagnostic tests and avail the benefit of modern techniques to remove birth defects wherever possible.
Periconceptional Care: The NFHS 3 data indicates gaps in timely antenatal care, highlighting the importance of periconceptional care. Integrating periconceptional counselling into existing primary health care infrastructure, particularly through the National Rural Health Mission, can effectively target potential risk factors early in the conception phase.
Public Health Initiatives: Initiatives like iron folic acid supplementation during pregnancy, universal iodization, and double fortification of salt and flour with essential nutrients have been initiated but need more widespread and consistent implementation. Fortification programs, as seen in the case of flour, require ongoing efforts to reach marginalized populations.
Birth Defects Registry: While the Birth Defects Registry of India provides valuable data, the reported prevalence of 84.2/10,000 in 2010 is significantly lower than estimated prevalence rates. Establishing more comprehensive, population-based registries, alongside utilizing existing nationwide surveys for data collection, is essential for a more accurate understanding of birth defect prevalence.
National Program for Hemoglobinopathies: Given the high carrier rates for haemoglobinopathies, a national program for thalassemia and sickle cell anaemia is critical. Identifying carrier status before reproduction or early in pregnancy allows for timely interventions, aligning with proven cost-effective strategies.











