- News |
-
- Featured
-
Canada’s privacy commissioner launches investigation over the use..
As the years pass by, technology also widens, and more and more are being discovered. From simple gadgets..
- Business |
-
- Featured
-
Be an informer to I-T dept; earn up..
Sharing "specific information" with the income tax department about any benami..

- Tech & Industry |
-
- Featured
-
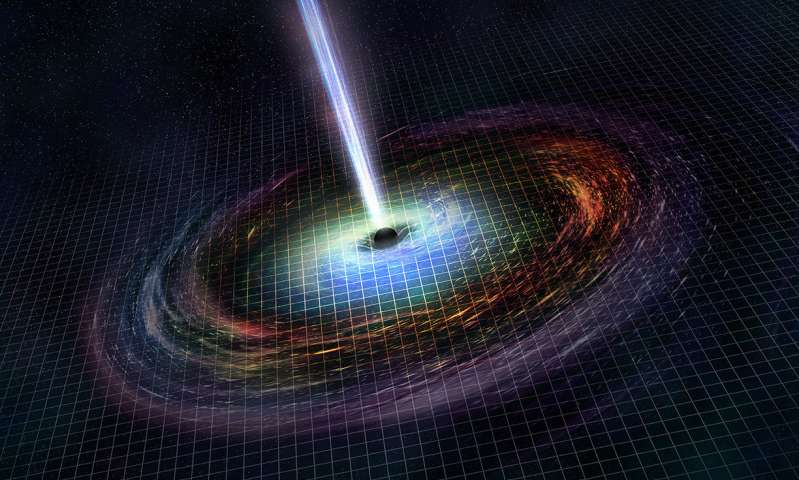
Gravitational wave event likely signaled birth of black..
The merger of two neutron stars that generated gravitational waves detected last year may have led to the birth..
- Entertainment |
-
- Topics
- Malayalam Film
- Media
- Music
- Youth
-
- Featured
-
Shawn Mendes Released Highly Anticipated Self-Titled Album Today
Los Angeles, CA : Multi-Platinum singer/songwriter Shawn Mendes released his highly anticipated self-titled third album today, via Island Records. Get..
-
- New Products |
-
- Topics
- General
-
- Featured
-
ZOTAC Introduces Its GeForce GTX 960 series graphics..
Dubai- ZOTAC International, a leading innovator and manufacturer of graphic cards and mini-

-
- Education |
-
- Topics
- Campus News
-
- Featured
-
ITM University, Gurgaon Student Palash Chhabra Represents Varsity..
New Delhi: Palash Chhabra, a student of ITM University,..

-
- Health |
-
- Topics
- Medical News
-
- Featured
-
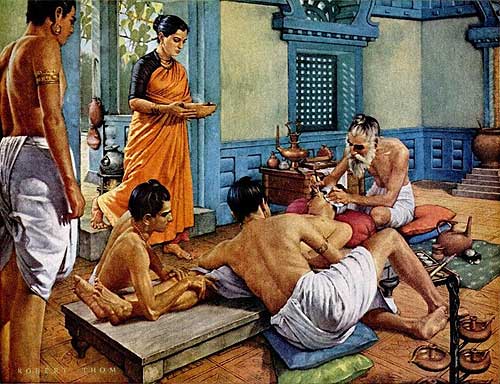
Maharshi Shushruta, The Great Grandfather of Surgery!
by Ayurvedacharya Dr.Hitesh Jani Dr.Hitesh Jani
-
- Tourism |
-
- Topics
- Travel
- Food&Beverages
- Hospitality
-
- Featured
-
“Keraliya Ayurveda is Credible and Authentic”
Irina Gurjeva Irina Gurjeva is not just another vacationer in..

-
- Sports |
- Editor's column |
- Magazine |
Retired Anesthesiologist Dr. Paul DeLeeuw Recalls the Only Loss In His Care
Published on December 6, 2022

Dr. Paul DeLeeuw currently works as a bariatric doctor helping patients to lose weight throughout Central and Southern Florida. However, he spent four decades of his career working as an anesthesiologist, until a shoulder industry forced him to retire from anesthesia in 2008. During his long career, which included many years as the Chief of Anesthesia at Cedars Medical Center in Miami, he has saved countless lives.
An avid storyteller, Dr. DeLeeuw often recounts the unusual circumstances and unique cases that he treated over the years. These include being called upon to save lives on an airplane, in a theater, and in his own kitchen, as well as complex surgeries in which he was pushed to his limits as a physician.
Like many doctors, Dr. Paul DeLeeuw is often asked if anybody has ever died while in his care. Surprisingly, his answer is, “I’m not sure.” There is one case in which he simply can’t be sure that the loss of a patient was due to his handling of the situation. An isolated incident in a successful 40-year career, Dr. DeLeeuw is certain that a surgery like this one would not be attempted today.
An Aggressive Cancer & Unsuccessful Surgery
Decades ago, a young wife and mother with aggressive colon cancer had been treated with a radical colectomy with excision of the lymph nodes and implantation of radioactive seeds. After surgery, she then went through several courses of chemotherapy and was declared cancer-free.
It was two years later that the same young woman completed follow-up scans that detected cancer once again. A small, isolated mass was found in the liver and analyzed scans found that an ordinary surgeon would not be qualified to remove the cancer. After calling around for an exceptional surgeon, the celebrated “Dr. Ragus Rakab” agreed to perform the surgery, with conditions. He would only accept cash and must have his own assistants, scrub nurse team, and instruments. However, he left the anesthesia to just anyone, which fell to Dr. DeLeeuw.
The night before the surgery, Dr. Paul DeLeeuw visited with the patient. She was clear in her request that, “if it looks bad, please let me die.” This wasn’t the first time that a patient had said such a thing to Dr. DeLeeuw, but he could not honor the request. His job never changed: to keep the patient alive. He was sure of it and he never wavered from it.
During surgery, Dr. DeLeeuw would monitor and manage a patient’s breathing, oxygen, blood pressure, bleeding, relaxation, electrolytes, and a dozen other variables. Although exhausting and all-consuming, this is the job of the anesthesiologist. To give up and let a patient go was not an option.
Going into the surgery, Dr. DeLeeuw understood that massive blood loss was to be expected. The liver is like a sponge filled with blood vessels from three different systems, and ordinary surgeons do not dare touch it. “Dr. Rakab” had completed surgeries like this one, but for Dr. DeLeeuw this was the first. He made a robust order from the Blood Bank, including blood, plasma, clotting factors, platelets, and anything else he may find a use for.
Before the surgery began, Dr. Paul DeLeeuw inserted two specialty catheters into the patient. A fine catheter in the wrist allowed him to monitor her blood pressure beat-to-beat, no matter how high or low it got. A catheter in the neck attached to fluid and recorded venous pressure, with a third connector allowing him to pump a whole unit of blood, a pint, into the patient in one minute. The surgery was ready to begin.
The liver is located under the right ribs and is highly inaccessible. “Dr. Rakab” and his assistants got to work, but it wasn’t long before they ran into trouble. Bleeding began and only worsened. Two units of blood were lost, and the tumor was encased in a swarm of blood vessels, unable to be cut out.
“Dr. Rakab” announced that he would be removing the liver, which was a radical decision. The liver is broken into two parts, so he would be removing the one with the tumor, which exposed more and bigger blood vessels. It became impossible to determine how much blood was lost. Dr. DeLeeuw pumped blood in as fast as the Blood Bank could supply it, infused with Fresh Frozen plasma for clotting factors and packets of platelets to help control bleeding.
It was a losing battle. The patient’s blood pressure was low and getting lower; her venous pressure was low.
Finally, “Dr. Rakab” declared that he could not control the bleeding. This was a first for Dr. DeLeeuw. He had no idea how to respond. What should he do?
“Dr. Rakab” removed his packing, packed up his instruments, filled the exposed tissues with absorbable clotting material, and began to close the abdomen. The surgery was over.
The cancer had not been removed. The patient was alive but bleeding internally. But Dr. DeLeeuw had done his job to the best of his ability, and now the patient was so full of blood and blood products that her body refused to die.
The patient was transported to the ICU, where Dr. DeLeeuw gave her a long-lasting narcotic that would allow her to remain unconscious until the end. Her fate was inevitable, but she would not suffer.
She died three hours later in the ICU.
The patient’s family was relieved to hear that there was no suffering but refused to pay the surgeon’s bill.
A Tragic Loss
Dr. Paul DeLeeuw has never forgotten this unique scenario, in which he worked outside of his comfort zone and to the height of his abilities, only to end in failure. Although the tragic loss of the patient can not be attributed to his care, the circumstances that he was subjected to left him with few options.
In a four-decade-long career with no other losses, this remains the one major disappointment for Dr. Paul DeLeeuw.









